

Abstract
Background: High incidence of graft failure is a major obstacle for successful unrelated cord blood transplantation (UCBT). To ensure engraftment, unrelated cord blood (UCB) unit with higher total nucleated cell (TNC) and CD34 cell doses and less HLA mismatches between UCB units and patients were usually selected. However, it remains unclear whether HLA haplotype between the UCB units and patients should be matched. Using data from Japanese registry, we analyzed the effect of haplotype matching on the outcomes after single UCBT.
Methods: Patients with hematologic diseases, aged 16 years or more, and have undergone their first UCBT between 2005 and 2014 were included in the study. The effect of haplotype matching (0, 1, and 2 haplotype matches) on neutrophil engraftment, overall mortality, relapse, and non-relapse mortality was analyzed after adjusting for other significant variables. Haplotype was estimated based on HLA-A, -B, -C, and -DRB1 allele information and Japanese allele frequency data. The haplotypes of both the patient and UCB unit were determined in 1,347 cases. Cases with more than 4 allele mismatches (n = 96) were excluded from the study.
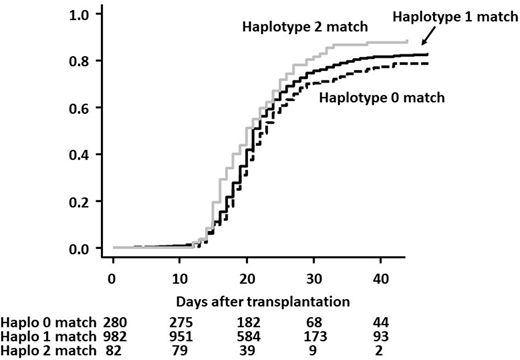
Results: The median age of the patients included in the study was 55 years (range 16-79 years). Median TNC and CD34 doses were 2.7 x 107/kg (range, 1.4-8.1x107/kg) and 0.8 x 105/kg (range, 0.1-5.2x105/kg), respectively. The number of allele mismatches were 0 in 82, 1 in 154, 2 in 252, 3 in 565, and 4 in 294 patients. The graft-versus-host disease (GVHD) prophylaxes were calcineurin inhibitors in combination with methotrexate in 707, calcineurin inhibitors in combination with Mycophenolate mofetil in 430, and other prophylaxes in 208 patients. The cumulative incidence of neutrophil engraftment at day 42 among groups with 0, 1, and 2 HLA haplotype matches was 79%, 82%, and 88%, respectively (Gray test, P=0.008) (Figure 1). In the multivariate analysis, the group with no haplotype match was marginally associated with worse neutrophil engraftment compared to the group with 1 haplotype match group (0 match vs. 1 match, HR 0.88, P=0.087), whereas the group with 2 haplotype matches was significantly associated with better neutrophil engraftment (2 match vs. 1 match, HR 1.39, P=0.005). Other significant variables were recipient sex, CD34 cell dose, transplant year, performance status, ABO matching, GVHD prophylaxis, and disease status. Tendency of worse neutrophil engraftment in the group with no haplotype matches was more apparent in patients with double mismatches at the same locus (0 match + no double mismatch vs. 1 match, HR 0.93, P=0.429, 0 match + double mismatch vs. 1 match, HR 0.80, P=0.050). Haplotype matching did not have any effect on overall survival and non-relapse mortality. Group with 2 haplotype matches was significantly associated with higher risk of relapse than the group with 1 haplotype match, whereas, there was no difference in the risk of relapse between the groups with no match and 1 match.
Conclusions: In addition to the CD34 cell dose and HLA matching, HLA haplotype matching might be considered to obtain better neutrophil engraftment. Two haplotype matches (8 of 8 allele matches) should be avoided if the relapse risk is high.
Tanaka:Pfizer: Honoraria; Otsuka: Honoraria; Bristol-Myers Squibb: Honoraria, Research Funding; Novartis Pharma: Honoraria. Ichinohe:Zenyaku Kogyo Co.: Research Funding; Celgene: Honoraria; Janssen Pharmaceutical K.K.: Honoraria; Taiho Pharmaceutical Co.: Research Funding; Mundipharma: Honoraria; Otsuka Pharmaceutical Co.: Research Funding; Nippon Shinyaku Co.: Research Funding; Sumitomo Dainippon Pharma Co.: Research Funding; MSD: Research Funding; Novartis.: Honoraria; JCR Pharmaceuticals: Honoraria; Alexion Pharmaceuticals: Honoraria; Repertoire Genesis Inc.: Research Funding; Bristol-Myers Squibb: Honoraria; Takeda Pharmaceutical Co.: Research Funding; Pfizer: Research Funding; Ono Pharmaceutical Co.: Research Funding; Kyowa Hakko Kirin Co.: Research Funding; Eisai Co.: Research Funding; CSL Behring: Research Funding; Chugai Pharmaceutical Co.: Research Funding; Astellas Pharma: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal